

Consent to Treatment
Welcome to Dua Health. This document contains important information about our policies and professional services. Please read it carefully and discuss any questions you have with your provider.
Our providers are affiliated with the following professional entity: Dua Health Group PLLC, a Texas professional limited liability company. In this document, the terms “we,” “us,” or “our” refer to Dua Health Group PLLC and any providers practicing through it. The terms “you” and “yours” refer to the individual(s) receiving services from our providers.
Our Notice of Privacy Practices, the policies outlined in this document, as well as applicable federal and state laws, apply to both in-office and teletherapy services, regardless of modality.
By signing this document, you, or the person authorized to act on your behalf, affirm your agreement to the policies contained herein and your consent to receive professional services. Your consent to treatment remains valid until your patient relationship with Dua Health is formally terminated.
Psychotherapy Services
Psychotherapy, often called talk therapy, is a form of treatment that can be helpful to individuals. There are many different definitions and philosophies of psychotherapy, and each of our providers will offer their own unique approach to treatment in alignment with your goals, desires, and preferences. Therapy may be provided as individual therapy or relationship therapy for couples or adult family members.
Therapy has both benefits and risks. Benefits can include improved mood, better relationships, and resolution of specific issues. However, therapy is not guaranteed to work for everyone. It may involve exploring difficult or painful aspects of your life and, at times, may lead to feelings of discomfort (e.g., guilt, anxiety, frustration, etc.) or a temporary increase in symptoms. These effects are usually temporary but should be openly discussed with your provider.
Your course of treatment will be tailored to your individual needs based on the intensity and duration of your concerns, your level of engagement and participation, and the specific nature of the issues being addressed. If you have any questions about the approaches used during your therapy, including possible risks, alternatives, your provider’s qualifications, or the treatment plan in general, please speak with your provider at any time.
You have the right to withdraw from treatment at any time. However, it is strongly encouraged that you discuss your desire to end treatment with your provider before doing so. This allows them to offer final recommendations or appropriate referral options. If at any point your provider determines that sessions are no longer effective in helping you meet your goals, they will discuss this with you and may recommend ending treatment and suggest other services or providers.
If you commit an act of violence or verbally or physically threaten or harass your provider, their colleagues, family members, or anyone affiliated with Dua Health, your provider reserves the right to immediately and unilaterally terminate treatment. Persistent failure or refusal to pay for services after a reasonable period is another valid reason for termination of services.
Dua Health
Therapist Qualifications and Supervision
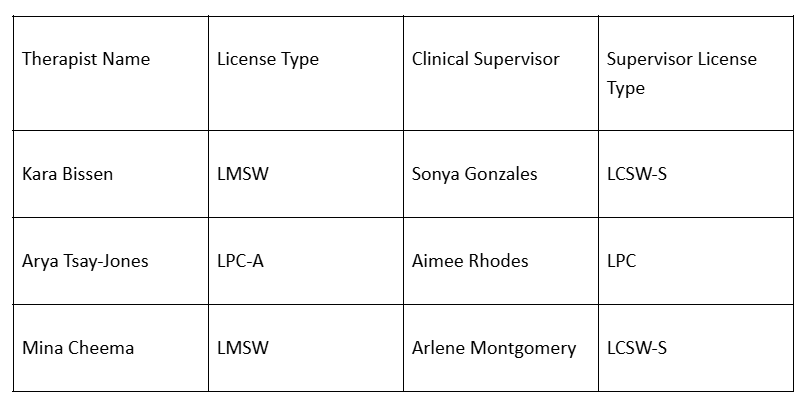
At Dua Health, we employ licensed clinicians and associate therapists who provide counseling services in accordance with the laws and ethical standards of the State of Texas. Associate therapists are provisionally licensed professionals, such as Licensed Master Social Workers (LMSW) or Licensed Professional Counselor Associates (LPC-Associates).
As provisionally licensed practitioners, associates are not independently licensed to practice counseling or psychotherapy. They are required by the Texas State Board of Examiners to engage in ongoing clinical supervision with a board-approved supervisor.
As part of their training and professional development, associate therapists meet regularly with their assigned clinical supervisors to review cases, treatment plans, and client progress. This supervision ensures the delivery of ethical and effective clinical care. All information shared with supervisors is treated as confidential and adheres to the same standards of privacy applicable to your treatment.
Clinical Supervision Information
All information shared with supervisors is maintained in accordance with HIPAA privacy and confidentiality standards.
Billing Supervision
Our billing supervisor is Agha Hussain.
All billing-related inquiries or insurance questions should be directed to:
careteam@duahealth.co
(512) 270-0044
Our billing supervisor oversees the administrative and financial processes related to client services, including insurance claims, payment reconciliation, and coordination with payers. They do have access to clinical notes and confidential patient information to review the notes before they sign the chart.
Consent and Acknowledgment
I have read and understood the information provided above. My therapist has explained the process of counseling and answered all my questions to my satisfaction. I understand that associate therapists work under the supervision of licensed clinical supervisors.
By signing below, I voluntarily consent to receive counseling services with Dua Health.
Couples Therapy (if applicable)
If you are participating in couples therapy, one person will be designated as the Identified Patient for clinical documentation and billing purposes. The Identified Patient is the individual whose insurance will be billed, if applicable, and whose information is maintained in our records.
By participating in couples therapy:
You acknowledge that both partners are voluntarily participating in treatment.
You understand that only the Identified Patient is considered a formal client of record.
Your provider adheres to a “no-secrets” policy, meaning relevant information disclosed individually may be shared within the couple’s sessions if clinically appropriate.
You consent to limited confidentiality between partners for the purposes of shared therapeutic goals.
The non-Identified Partner will not have access to the clinical record or be billed for services, and does not retain independent rights under HIPAA as a patient.
If you are the non-Identified Partner, you will be asked to sign a separate one-page consent acknowledging these terms.
Family Therapy Participation (if applicable)
In family therapy, multiple individuals may participate in shared sessions. One person will typically be designated as the *Identified Patient* for purposes of clinical documentation and billing.
Each family member may be asked to sign a limited consent acknowledging participation in shared sessions.
Only the Identified Patient will have a formal treatment record; other participants are not considered clients of record unless individual sessions are requested and agreed upon separately.
Family members agree to shared confidentiality, meaning that information discussed in joint sessions may be heard by all participants.
Providers do not act as neutral mediators or legal advocates in family conflicts and may not be appropriate for court-involved cases.
Minors and Parent/Guardian Participation (if applicable)
When providing therapy to a minor, the parent or legal guardian will be asked to sign all initial consents. In accordance with applicable law and clinical judgment:
Parents may participate in sessions as needed to support the minor’s care.
The provider may recommend limited or full confidentiality between the minor and provider, depending on age, maturity, and presenting issues.
Providers will not automatically share all details of the minor’s therapy with parents but may disclose safety concerns, treatment recommendations, or relevant updates.
Any exceptions to confidentiality will be discussed with both the parent/guardian and minor when appropriate.
Legal Custody: We require that a parent or guardian with legal custody complete intake and consent forms. You may be asked to provide documentation of custody if needed.
Confidentiality: Our providers aim to create a safe therapeutic environment for minors. In many cases, particularly with adolescents, we may limit the information shared with parents to promote open communication and emotional safety. We will always share concerns related to safety, harm to self or others, or abuse.
Parental Involvement: Parents may be invited to participate in portions of sessions or in separate parent-only sessions if clinically appropriate.
Legal Proceedings: Dua Health providers do not provide forensic evaluations, custody recommendations, or court testimony. We are not considered neutral evaluators and reserve the right to decline participation in legal proceedings related to the minor’s care.
Please inform us of any active legal matters involving your child so we can determine whether services are appropriate.
Confidentiality
Your privacy is important. In general, the privacy of all communications between a patient and a provider is protected by law, and providers can only release information about their work with a patient with the patient’s written permission. However, there are a few important exceptions.
In certain circumstances, your provider is required by law to notify legal authorities or potentially affected individuals in the following situations:
If there is suspected abuse or neglect of an elder, incapacitated, or dependent adult, or child.
If, in your provider’s judgment, you are in danger of harming yourself or another person, or are unable to care for yourself.
If you communicate to your provider a serious threat of physical violence against another person.
Additional limits to confidentiality include:
If your provider is ordered by a court to release information as part of a legal proceeding, they may be required to share details of your care.
Your provider may, on occasion, consult with other professionals in their areas of expertise to provide the best treatment for you. In such cases, information may be shared without identifying you by name.
If your provider reasonably believes you are experiencing a psychiatric emergency, they may initiate a welfare check or contact your designated emergency contact.
As otherwise required by law and/or outlined in our Notice of Privacy Practices.
It is also important to note that your provider adheres to a “no-secrets” policy for relationship therapy. This policy will be reviewed with you during your initial session. If you have questions about the “no-secrets” policy, please ask your provider at any time.
No one is permitted to record a session.
While this written summary of exceptions to confidentiality should be helpful in informing you about potential limitations, it is important that you bring up any questions or concerns with your provider directly.
Attendance and Cancellation
Consistency is essential for the overall progress and effectiveness of therapy. Please be on time for your scheduled appointment. Appointments must be canceled or rescheduled at least 24 hours in advance to avoid any charges. You will be considered a no-show if you are more than 15 minutes late to your scheduled appointment. To reschedule or cancel an appointment, please contact hello@duahealth.co.
If you cancel with less than 24 hours’ notice or miss your scheduled appointment, you will be charged a cancellation fee. This cancellation fee is not eligible for insurance reimbursement.
Your provider is often not immediately available by telephone. If you need to contact your provider between sessions for non-urgent issues, please contact hello@duahealth.co.
Billing and Payments
We require payment at the time of service. This includes any applicable copay, coinsurance, or deductible. This consent authorizes us to charge your credit card on file for services rendered and to submit billing claims to your insurance company, health plan, or third-party administrator for reimbursement.
We may update our fees as needed, including at the beginning of each calendar year. All fees are subject to change with 30 days’ written notice.
If you have any questions, please contact us at hello@duahealth.co.
Teletherapy
Services may be provided to you in-person or through teletherapy technologies, as deemed clinically appropriate. This consent provides you with important information about teletherapy. By signing this consent, you agree to participate in teletherapy and receive services from your provider via synchronous and/or asynchronous technologies, as appropriate.
Teletherapy refers to psychotherapy services provided digitally—typically via secure video conference, but in some circumstances via telephone. Teletherapy offers an effective option for continuity of care when in-person sessions are not possible or not preferred. You are not required to receive services via teletherapy and may withdraw your consent at any time.
Your provider will be licensed in the state where you are located when services are rendered, or will otherwise meet a licensure exception permitted by applicable state law. The provider will establish a provider-patient relationship in accordance with relevant state laws and regulations. Please inform your provider if you will be traveling to, or moving to, another state. In some cases, providers may not be able to continue services while you are in another state, even temporarily.
The benefits of teletherapy include:
Easier access to care and continuity of care
Convenience of meeting from your preferred location (subject to applicable laws)
The potential risks of teletherapy include:
Interruptions, background noise, or technical difficulties
Unauthorized access to your health information if you are not in a private location
Inability of your provider to provide immediate in-person support in the event of a crisis
If you are unable to communicate with your provider due to technological issues, please contact support@duahealth.co.
During the course of treatment, it may be helpful to communicate with you via email, text message, or other electronic means. By signing this consent, you agree to receive periodic electronic communications (e.g., emails, calls, or texts) from us about the services you have received or will receive. You may opt out at any time. While your provider will make reasonable efforts to protect the privacy and security of all electronic communications—including those conducted through teletherapy—we cannot guarantee complete confidentiality through these channels.
Death or Incapacity of Provider
In the event that your provider becomes incapacitated or dies, it may be necessary for another provider to take possession of your file and records. By signing this form, you consent to allow another licensed professional designated by your provider or Dua Health to take possession of your file and records. Upon request, your records may be provided to you or transferred to a provider of your choice.
Research, Writing, Teaching
Your provider and other team members at Dua Health may engage in internal research and training, or publish information for professional or public audiences. De-identified or anonymized information about you and your treatment may be used to support these efforts. No identifying information will be disclosed. Any such use will strictly adhere to standards of privacy and confidentiality.
Emergencies
IF YOU ARE IN A STATE OF CRISIS OR EMERGENCY, PLEASE DIAL 911 OR GO TO THE LOCAL EMERGENCY ROOM. IN THE EVENT YOU ARE EXPERIENCING EMOTIONAL DISTRESS, PLEASE CALL OR TEXT 988, THE SUICIDE AND CRISIS LIFELINE.
If you have any questions or concerns regarding this document, please speak to your provider or contact support@duahealth.co.
Notice of Privacy Practices
OUR PRIVACY COMMITMENT
Thank you for giving us the opportunity to serve you. In the normal course of doing business, Dua Health LLC, on behalf of Dua Health Group PLLC, creates, obtains, and/or maintains records about you and the services we provide. The information we collect is called protected health information (“PHI”). We take our obligation to keep your PHI secure and confidential very seriously.
We are required by federal and state law to protect the privacy of your PHI and to provide you with this Notice of Privacy Practices (“Notice”) describing how we safeguard and use your PHI, and how we will notify you following a breach of your unsecured PHI.
When we use or disclose your PHI, we are bound by the terms of this Notice. This Notice applies to all electronic or paper records we create, obtain, and/or maintain that contain your PHI.
THIS NOTICE DESCRIBES:
How we may use and disclose your PHI
Your rights to access and amend your PHI
WE ARE REQUIRED BY LAW TO:
Maintain the privacy of your PHI
Provide you with this Notice of our legal duties and privacy practices with respect to PHI
Abide by the terms of this Notice
HOW WE PROTECT YOUR PRIVACY
We understand the importance of protecting your PHI. We maintain technical, physical, and administrative safeguards to ensure the privacy and security of your information.
PERMITTED USES AND DISCLOSURES OF YOUR PHI
HOW WE MAY USE PHI WITHOUT YOUR AUTHORIZATION
Treatment – We may use and disclose your PHI to healthcare professionals or other third parties to provide, coordinate, and manage the delivery of healthcare. For example, behavioral health assessments and other PHI may be disclosed to your health insurer or your primary care provider to support the provision of behavioral health services.
Payment – We may use and disclose PHI about you to receive payment for our services, determine your insurance eligibility or coverage, manage your account, fulfill benefit plan responsibilities, and process claims for services rendered. For example, we may disclose PHI to your health plan or employer (or their designees) to verify eligibility or submit claims for reimbursement.
Healthcare Operations – We may use and disclose your PHI for our internal operations, such as quality assessment, staff training, auditing, utilization review, and other necessary administrative activities. For example, we may use your PHI to assess treatment outcomes, develop clinical protocols, or improve our services.
Disclosures to Your Employer as Sponsor of Your Health Plan – Where permitted by law, we may disclose your PHI to your employer or a vendor acting on its behalf to administer your employee health plan. Your employer may not use your PHI for any purpose other than plan administration. Please refer to your health plan documents for details on whether your employer receives PHI and, if so, who may access it.
Information That May Be of Interest to You – We may use or disclose your PHI to inform you about treatment options or other health-related services that may be of interest to you.
Individuals Involved in Your Care or Payment for Your Care – We may disclose PHI to a family member, friend, or other person involved in your care or payment for your care, unless you notify us in writing not to do so. We will request adequate verification of the individual’s authority to act on your behalf.
Legal Guardians – If you are under a legal guardianship, we may disclose your PHI to your legal guardian as required or permitted under federal or applicable state law.
Business Associates – We may share PHI with business associates who perform services on our behalf (e.g., billing, IT, analytics). Business associates are bound by contractual obligations to safeguard your PHI. If a business associate uses subcontractors, they must also enter into binding confidentiality agreements to ensure the continued protection of your information.
Research - Under certain circumstances, we may use and disclose PHI about you for research purposes. Before we use or disclose PHI for research, we will either remove personally identifying information, obtain your written authorization, or gain approval through an appropriate review process that ensures the protection of your privacy. In some cases, we may use your PHI to generate aggregate data (summarized data that does not personally identify you) to study outcomes, costs, or provider performance, or to help design benefits for employers or health plans. This aggregate data may be sold or disclosed to other organizations, but it will not personally identify you.
Abuse, Neglect, or Domestic Violence - We may disclose your PHI to a social services or protective agency or to another government authority if we believe you are a victim of abuse, neglect, or domestic violence. We will inform you of the disclosure unless doing so would place you at serious risk of harm.
Public Health - We may disclose your PHI for public health activities and purposes. These may include regulatory reporting, such as reporting adverse events, supporting vaccination efforts, preventing or controlling communicable diseases, or conducting post-marketing surveillance in connection with FDA mandates or product recalls.
We may receive payment from a third party for making certain public health-related disclosures.
Judicial and Administrative Proceedings - We may disclose your PHI in the course of any judicial or administrative proceeding if required by a court order, subpoena, or other lawful process—provided reasonable efforts have been made to notify you of the request or to obtain a protective order.
Law Enforcement - We may disclose your PHI as required by law in response to a subpoena, warrant, summons, or similar process. We may also provide information to assist law enforcement in identifying or locating a suspect, witness, or missing person; reporting a crime; providing details about a decedent; or when there is a concern for the safety of others.
Coroners and Medical Examiners - We may disclose PHI to a coroner or medical examiner to identify a deceased individual, determine cause of death, or perform other authorized duties.
Organ, Eye, and Tissue Donation - We may disclose PHI to organizations that facilitate organ, eye, or tissue donation and transplantation.
Workers’ Compensation - We may disclose your PHI to comply with workers’ compensation laws or similar programs that provide benefits for work-related injuries or illnesses.
Specialized Government Functions, Military, and Veterans - We may disclose your PHI to authorized federal officials to carry out lawful intelligence, counterintelligence, national security activities, or medical suitability determinations. If you are a member of the U.S. armed forces (or a foreign military), we may release your PHI as required by military command authorities or applicable law.
If you are incarcerated or in the custody of a law enforcement official, we may release your PHI if necessary for:
Providing health care services
Maintaining the health or safety of yourself or others
Ensuring the safety and security of the institution or its staff
As Otherwise Required by Law - We will disclose your PHI when required to do so by applicable federal, state, or local laws. If the law in your jurisdiction provides additional protections against the use or disclosure of PHI, we will follow those laws as applicable.
Health Oversight - We may disclose PHI to a health oversight agency for activities authorized by law, such as audits, investigations, licensure, or disciplinary actions. These agencies may oversee the healthcare system, public benefit programs, and compliance with civil rights laws.
Creation of De-Identified Health Information - We may use your PHI to create de-identified information by removing identifying details such as your name, address, and member ID. This de-identified data may be used for internal business purposes, such as generating summary reports or analyzing healthcare trends.
To Avert a Serious Threat to Health or Safety - We may disclose PHI if necessary to prevent or lessen a serious and imminent threat to your health or safety, or the health and safety of another person or the general public. Such disclosures will be made only to those who are reasonably able to prevent or reduce the threat.
OTHER USES AND DISCLOSURES OF PHI
Uses of PHI That Require Your Authorization
Most uses and disclosures of psychotherapy notes (where applicable), disclosures for marketing purposes, and disclosures that constitute a sale of PHI require your written authorization. These activities—and any other uses and disclosures of your PHI not otherwise described in this Notice—will be made only with your written authorization unless permitted by applicable law. You may revoke your authorization in writing at any time unless we have already acted in reliance on it.
Written revocation of authorization must be sent to the address listed at the end of this Notice.
Additional Protections for Certain Categories of PHI
Certain types of PHI may be subject to additional protections under federal or state law. This includes, but is not limited to:
Psychotherapy notes
PHI related to alcohol and drug use, diagnosis, and treatment
PHI concerning HIV/AIDS status, testing, or treatment
PHI related to venereal or other communicable diseases
PHI derived from genetic testing
Where applicable, we will comply with enhanced privacy protections as required by law.
YOUR RIGHTS WITH RESPECT TO YOUR PHI
You have the following rights regarding the PHI we maintain about you:
Right to Inspect and Copy
You may request to inspect and copy PHI that may be used to make decisions about your care, including records of enrollment, payment, claims adjudication, and case or medical management. If these records are maintained electronically, you may request them in electronic format. You may also request that we send your PHI to a third party, such as a Health Information Exchange (HIE). We may charge a reasonable fee to cover copying, mailing, or other associated costs. In certain circumstances, access may be denied as allowed by law.
Right to Amend
If you believe your PHI is incorrect or incomplete, you may request an amendment. You must provide a reason supporting your request. We may deny your request under certain conditions, and if we do, you may file a statement of disagreement. If the information was created by another provider or facility, we may refer you to them.
Right to an Accounting of Disclosures
You have the right to request an accounting of certain disclosures of your PHI made by us, excluding disclosures made:
To you
With your written authorization
For treatment, payment, or healthcare operations
Earlier than six years prior to the date of your request (or three years for electronic health records, if applicable)
As otherwise excluded by law
If you request more than one accounting in a 12-month period, we may charge a reasonable fee for each additional report.
Right to Request Restrictions
You may request limitations on how we use or disclose your PHI for treatment, payment, or healthcare operations. You may also request that we not share PHI with family members or friends involved in your care. We are not required to agree to your request, unless it relates to a disclosure to a health plan for payment or operations purposes (not treatment) and the PHI pertains to a service that you paid for entirely out-of-pocket.
Right to Confidential Communications
You may request that we communicate with you in an alternative way or at an alternative location to protect your confidentiality. Your request must include the method or location you prefer.
Right to Be Notified of a Breach
You have the right to be notified in the event of a breach of your unsecured PHI.
Right to a Paper Copy of This Notice
You have the right to request a paper copy of this Notice at any time, even if you have agreed to receive it electronically. To request a copy or obtain answers to frequently asked questions, please contact support@duahealth.co.
Right to File a Complaint
If you believe your privacy rights have been violated, you may file a complaint with us or with the U.S. Department of Health and Human Services. We will not retaliate against you for filing a complaint.
To submit written requests or complaints, please contact:
Dua Health LLC
Attn: Privacy Office
5900 Balcones Drive, Suite 100
Austin, TX 78731
hello@duahealth.co
Please include your name, mailing address, and any relevant identifiers.
ACKNOWLEDGEMENT OF NOTICE OF PRIVACY PRACTICES
The purpose of this form is to verify that you received this Notice of Privacy Practices. You are not required to sign or return the form.